
Read this 170 page PDF file first
Anatomy
Meibomian glands are the oil-producing glands located in both the upper and lower eyelids. They number about 25 to 30 (each: a total of about 100) and normally slowly release oil into the tear film. This oil helps to stop the water in the tears from evaporating, thus helping to prevent dry eyes. Detailed anatomy here.
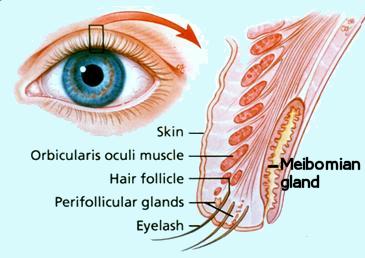
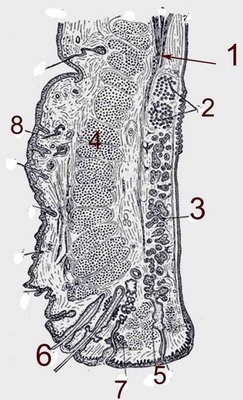
The meibomian glands (3 Fig above) of the tarsal plate produce the lipid that will line the layer of the tear film. The Meibomian lids empty into ducts that dot the marginal surface of the eyelid and can be seen emanating droplets of oil for the tears.
Normal glands:
Healthy
The cure for eye strain/ dry eyes (for most cases of dry eye) |
Over time, some of these glands die or otherwise atrophy. See this. Hyperkeratinization of ductal epithelium and atrophy of acinar cells may cause meibomian gland dysfunction.
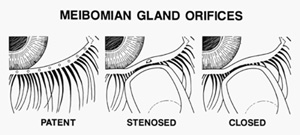
the natural history of MGD starts with hyperkeratinization of the duct epithelium leading to duct occlusion. This is seen as pouting or plugging of the gland orifices and production of keratin rich expressed material. This plugging causes damming back of the gland secretions that leads to disuse atrophy of the acini. In the advanced stages periductal scaring occurs, it is seen as an exaggerated opaque ring shaped opacity around the ducts or a focal absorption of the gland orifices that ends in total
damage and gland loss [Source]
MGD as a MAJOR CAUSE OF DRY EYES (Evaporative dry eyes)
Many people who have dry eye symptoms are treated as though the cause is aqueous deficiency (artificial tear supplementation and punctal plugs), when in fact their primary problem is meibomian gland dysfunction MGD. Some researchers believe that up to 70% of chronic dry eye may actually be MGD, not “classic” dry eye. More broadly, nearly half of the subjects with dry eyes have MGD [Academic paper].
Posterior blepharitis is often called meibomitis or meibomian gland dysfunction [Source]. Meibomian gland dysfunction is quite common and unfortunately it often goes undiagnosed. Even when diagnosed is often not treated or is not treated effectively until it has become chronic or severe.
MGD may be inflammatory (often as a result of blepharitis) or atrophic.
Blockage
Severe blockage can lead to much enlarged glands (a cyst) or even infection. It is therefore important to firstly, unclog the glands which are blocked and secondly to prevent them from blocking up again as much as possible
Thickening of oil
The oil is supposed to be nice and warm and runny, but sometimes it can get thick and gets stuck. This leads to blockage of the narrow duct which takes the oil from the gland to the tear film. The oil continues to be made and this can lead to filling and swelling of the glands.
reduces the eye’s ability to flush bacteria from the lid margins, enabling bacteria to infect the meibomian glands and eyelash follicles, in turn further degrading the tear film. In addition to aqueous deficiency dry eye, MGD contributes significantly to ocular surface disease. Since it is not always easy to distinguish the clinical signs and symptoms of MGD from dry eye disease or ocular allergy, the MGD may go untreated. [Source]
orifices progress from open to stenosed to closed (Figure below). [Source]
Symptoms
Cure
1. Unblock the glands
- Hold this against the closed eye for about one minute or so (see figure One).
- Then, having liquefied the oils with this warming, press with one finger firmly on your cheek.
- Next, with the first-finger, press firmly on the lower lid, pushing upward to push the oil up into the tear film (see figure Two).
- Do this a few times over the entire lower eyelid, and then repeat for the upper eyelid.
- Repeat the entire procedure for the other eye.
- Do this initially once per day for one week. This will help to unclog the blocked glands.
- After the first week, doing this once or twice per week should help prevent the glands from becoming reblocked.
efficacy—they do not penetrate the lid margin well, and most lack the needed antiinflammatory effect. While more effective, oral tetracyclines
often have unpleasant gastrointestinal side effects. [Source]
[See video below]
pressure and resulting dilatation of the ducts and in atrophy of the acini with rarefaction of the secretory meibocytes and gland dropout. Stasis can also increase the growth of commensal bacteria, their production of oil degrading enzymes and release of toxic mediators. These factors can act as self-enforcing feedback loops that aggravate the primary hyper-keratinization and compositional disturbance of meibum and can hence lead to a progressive MGD (Knop and Knop, 2009b). [Source]
Ophthalmology & Visual Science (IOVS) journal. The report is the result of findings from a two-year-long workshop composed of more than 50 leading clinical and basic research experts from around the world.
characterized by terminal duct obstruction and/or qualitative/quantitative changes in the glandular secretion. This may result in alteration of the tear film, symptoms of eye irritation, clinically apparent inflammation, and ocular surface disease.
needs of clinicians and researchers alike. The consensus paper further proposes recommendations for diagnosing MGD and MGD-related disorders and presents a sequence of diagnostic tests to be performed in an order that will minimize the extent to which one test influences those that follow.
far-reaching impact on the clinical care of patients, the group of experts concur that additional research be conducted to further study other aspects of MGD. These include its association with dry eye disease and standardized and validated ways to identify symptoms and signs of MGD.





